Everyone will eventually experience brain death. See more brain pictures.
Photo courtesy NASA
Many recent advancements in modern medicine and breakthroughs in the understanding of human physiology have made it possible to separately and artificially maintain tissue viability without the impulses being transmitted by the brainor brain stem.
Due to the continual medical advancements, there will be more and more patients who are being maintained by ventilation support systems -- their body temperature, blood pressure, pulse, nutrition and fluid requirements are being artificially maintained, but they have a non-viable (dead) brain. These patients are brain dead without any hope of recovery or survival.
Advertisement
In this article, you'll learn about the diagnosis of "brain death" and how it compares with coma and cardiac death.
Nothing in this article should be construed as a treatment regimen or suggested treatment regimen for any particular patient. All patients with neurological injury and the next of kin of the patient should rely on their local neurosurgeon or neurologist for the best care plan for the patient.
The brain can survive for up to six minutes after the heart stops. Afterward brain death results when the entire brain, including the brain stem, has irreversibly lost all function.
HowStuffWorks.com
First, one must clarify that everyone dies of "brain death." Whether an old person suffers cardiac arrest resulting in the lack of oxygen and nutrients to the brain, or a younger person suffers a gunshot wound to the head resulting in brain death, it's the same diagnosis.
The brain controls all our bodily functions, but there are three things it cannot do:
Advertisement
It cannot feel pain. The brain can feel pain from all over the body, but not within itself.
The brain cannot store oxygen. A person can feel a lack of oxygen after only a few seconds. When someone stands up too quickly and becomes dizzy, this is an example of the loss of blood flow to the brain that can be sensed.
The brain cannot store glucose (blood sugar). Diabetics who give themselves too much insulin can drop their blood sugar level and faint, and without immediate glucose infusion the brain can die.
The brain can survive for up to about six minutes after the heart stops. The reason to learn cardiopulmonary resuscitation (CPR) is that if CPR is started within six minutes of cardiac arrest, the brain may survive the lack of oxygen. After about six minutes without CPR, however, the brain begins to die. (See How CPR Works to learn more about the procedure.) Prompt resuscitation allows the physician time to assess and treat the damaged brain. Medication and mechanical ventilation permit tissue oxygenation, but severe brain damage or a prolonged period without oxygen or glucose causes the death of the brain.
By definition, "brain death" is "when the entire brain, including the brain stem, has irreversibly lost all function." The legal time of death is "that time when a physician(s) has determined that the brain and the brain stem have irreversibly lost all neurological function."
The Injured Brain
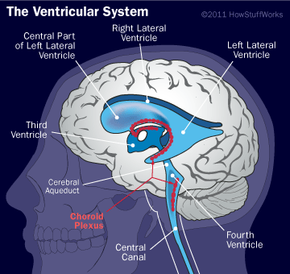
If pressure in the brain causes the ventricles to collapse, the results can be catastrophic.
When the brain is injured, whether by natural causes or trauma, there are three possible results: bleeding, swelling, or both. Causes for damage to the brain that may result in "brain death" include:
Trauma
Open (Gun shot wounds, etc)
Closed (Blunt injury, etc)
Anoxia (a period of no oxygen caused by drowning, hanging, smoke inhalation, carbon-monoxide poisoning, etc.)
Advertisement
Cerebral vascular accident
Stroke (emboli blocking arteries feeding the brain)
Bleeding in the brain can be catastrophic. Neurosurgeons can open the skull and try to control the bleeding. When the brain starts to swell, the ventricles collapse and the pressure within the skull starts to increase. The increasing intercranial pressure (ICP) must be treated or else major neurological problems occur. The physician will give the patient anti-inflammatory medications, high osmolar medication to reduce swelling and try to provide highly oxygenated blood, so any blood getting into the brain will produce the maximum benefit.
Even with everything being done to reduce bleeding and cellular swelling, the treatment may not be enough to control the ICP. As the ICP increases, there is nowhere for the swelling tissue to go because of the restrictions provided by the bony skull. Sometimes, the neurosurgeon will place a bolt into the skull. The bolt is screwed into the skull and has a hole in the middle, connected to a tube, which is used to remove some intercranial fluid, allowing for swelling and a way to measure the ICP.
If the ICP cannot be controlled, the pressure will continue until the ICP is the same as the patient's blood pressure. At this time, no blood will enter the brain, and the brain dies. In many cases, the pressure will increase to a point that the pressure will push the brain stem down into the spinal column. This is called brain herniation, and it results in instantaneous brain death.
Coma vs. Brain Death
Patients who suffer brain death are not in coma. Patients in coma may or may not progress to brain death.
The brain is a very complex organ. It is the brain that controls not only an individual's thought process and voluntary movements, but it controls involuntary movements and other vital body functions. These functions include auditory, olfactory, visual and tactile senses, regulation of body temperature, blood pressure, respiration, and heart rate (although the heart can continue to beat without the brain in "autotonic response"). The brain also produces hormones to control individual organ function. A good example is the brain's production of anti-diuretic hormone (ADH). This hormone is produced to concentrate the urine in the kidneys, thus protecting against life-threatening dehydration.
Advertisement
Patients in coma may be in deep coma or may survive in what is termed a "vegetative state." The difference between these two groups is that a deep coma patient usually requires hospital care, while a patient in a vegetative state may be released to the family for home care. The individual in the vegetative state has a lot more lower-brain function, and a bit more upper brain-stem function, than a patient in deep coma.
In either case, the patient is considered legally alive. Patients who are in coma will have some neurological signs. The amount of brain activity is variable, and extensive clinical examinations are performed on these patients. The physician(s) observes the patient for any sign of electrical impulse leaving the brain as a result of an external stimulus. Patients in coma will have these signs; patients who suffer brain death will not.
Examining for Brain Death
The examination for brain death is based on response to external stimuli. Since the brain is the organ that feels outside pain, when the brain is dead the patient feels nothing. Before the examination is performed, the physician will have a toxicology test performed to make sure the patient does not have any muscle relaxants in his system, and will check that the patient's body temperature is not extremely abnormal, either of which may reduce neurological reflexes.
The positive examination for brain death includes the following:
Advertisement
The patient has no response to command, verbal, visual or otherwise.
The patient is flaccid, with areflexic extremities. The patient has no movements -- the arms and legs are raised and allowed to fall to see if there are adjacent movements, restraint or hesitation in the fall.
The pupils are unreactive (fixed). The patient's eyes are opened and a very bright light is shined into the pupil. The light will activate the optic nerve and send a message to the brain. In the normal brain, the brain will send an impulse back to the eye to constrict the pupil. In the non-viable brain, no impulse will be generated. This is performed in both eyes.
The patient has no oculocephalic reflex. The patient's eyes are opened and the head turned from side to side. The active brain will allow a roving motion of the eyes; the non-functional brain will not. The eyes remain fixed.
The patient has no corneal reflexes. A cotton swab is dragged across the cornea while the eye is held open. The intact brain will want the eye to blink. The dead brain will not. This is performed in both eyes.
The patient has no response -- either purposeful or posturing -- to supra-orbital stimulation. The patient's eyebrow ridge is compressed with the thumb. The resulting stimulation pressure will cause motion of the extremities, either purposeful or primitive posturing, in the living-brain patient, but none in the brain-dead patient.
The patient has no oculovestibular reflex. The patient's ear canal is inspected to ensure an intact tympanic membrane and that the ear is free of wax. While holding the eyes open, ice water is injected into the ear canal. The drastic change in ear temperature will cause a violent eye twitching by the intact brain but no reaction in the brain-dead patient. This is performed in both ears.
The patient has no gag reflex. The movement of the breathing tube (in and out) or the insertion of a smaller tube down the breathing tube will cause a gag reflex in a comatose patient, but will not elicit a reflex in the brain-dead patient.
The patient has no spontaneous respiration. The patient is temporarily removed from life support (the ventilator). With the cessation of breathing by the machine, the body will immediately start to build up metabolic waste of carton dioxide (CO2) in the blood. When the CO2 level reaches a level of 55 mm Hg, the active brain will cause the patient to breathe spontaneously. The dead brain gives no response.
If, after this extensive clinical examination, the patient shows no sign of neurological function and the cause of the injury is known, the patient can be pronounced "brain dead." In some states, more than one physician is required to make this pronouncement in order for brain death to become legal death.
Although the patient has a dead brain and dead brain stem, there may be spinal cord reflexes that can be elicited (a knee jerk, for example). In some brain dead patients, when the hand or foot is touched in a particular manner, the touch will elicit a short reflex movement.
Many physicians will order a confirmatory test for brain death when the clinical examination demonstrates no neurological function.
Confirming Brain Death
HowStuffWorks.com
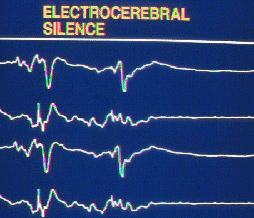
Many physicians request additional, confirmatory tests before pronouncing brain death. The two most common are the electroencephalogram (EEG) and the cerebral blood flow (CBF) study.
The EEG measures brain voltage in microvolts. It is so sensitive that the static electricity in a person's clothes will give a squiggle on the EEG (a false positive). All positive responses suggest brain function. The patient in the deepest coma will show some EEG electroactivity, while the brain-dead patient will not.
Advertisement
The cerebral blood flow (CBF) study study involves the injection of a mild radioactive isotope into the blood stream. By placing a radioactivity counter over the head, one can measure the amount of blood flow into the brain. (See How Nuclear Medicine Works.) The cerebral blood flow study takes 20 to 30 minutes to perform. If there is no blood flow to the brain as demonstrated by this study, the brain is dead. A negative cerebral flow study is indisputable evidence of a dead brain.
Normal cerebral blood flow study showing cranial space filled with bloodCerebral blood flow study showing no blood entering the brain
Another confirmatory test is chemical: The patient can be given 1 mg of atropine IV. In the patient with an intact brain, atropine will dramatically increase the patient's heart rate. In a brain-dead patient, atropine will not influence heart rate.
Now you have some idea of the scope of the examination that takes place before a patient is pronounced "brain dead." Patients are considered either alive or dead. One cannot be "almost" brain dead or "essentially" brain dead. Brain death, like pregnancy, is either "yes" or "no." Likewise, brain death is a very conservative diagnosis. It is not made lightly, but only when there is no doubt in the findings.
The criterion for the determination of death has always been left to physicians. The diagnosis of "brain death" is only possible because of modern medicine's ability to maintain the functions of supporting organs of the body after the brain is no longer viable. This support of the body is essential to evaluate the patient for possible survival and returning function of the brain. Once the examination of the brain has determined that it is no longer viable and there is no chance of any recovery of function, the "brain death" diagnosis is made.
Once a patient fulfills this medical criterion, nothing can be done for the patient. The patient can still be maintained physiologically on the ventilator, but there is no hope of any kind of recovery, even to a state of irreversible coma.
The brain performs many functions, including thought, movement and all the neurological function that allow the body to maintain blood pressure, heart rate, body temperature and organ function. When the brain dies, the body's organs will collapse. Massive artificial medical measures must be started to maintain organ function, but even in the best hands, these interventions are only a temporary measure.
Families of a brain dead patient must, by federal regulations, be provided the option of organ donation. If the family consents, the regional organ procurement organization is involved. If the family refuses, the mechanical ventilator, medications and fluids are discontinued, after which the heart stops.
Organ Donation
Heart transplant patient Jennifer Sutton donated her heart to promote awareness about organ donation and Restrictive Cardiomyopathy -- a disease that nearly killed her.
SHAUN CURRY/AFP/Getty Images
It is the brain-dead patient who is the source of viable organs for transplantation. If a family member knows that the patient wishes to be an organ donor, the best way to ensure that the patient's wishes are honored is for the family to approach the medical staff about it. This is why organ procurement organizations ask individuals who sign a donor card to inform their family of their wishes. When a family-initiated donation occurs, any and all obstacles in the donation process evaporate.
Brain death occurs in one out of every 200 hospital deaths (CDC study, 1986). It is a fairly rare event. These patients are evaluated for donation, with half being excluded because of other medical problems (cancers, infections, etc.). Of the half with medically acceptable organs, half of the families refuse donation, resulting in one organ donor out of 800 hospital deaths. To learn more about organ donation, see How Organ Transplants Work.
Advertisement
For more information on brain death and related topics, check out the links on the next page.
Leslie C. Olson is a surgical specialist at LifeCenter NW. LifeCenter NW is the Organ Procurement Organization based in Bellevue, Washington, serving Washington, Alaska, Northern Idaho & Montana.
Cite This!
Please copy/paste the following text to properly cite this HowStuffWorks.com article: