What happens when you're cutting a bagel and slice your hand with the knife? Besides all the blood, you'll probably feel an immediate sharp pain, followed by a longer-lasting dull ache. Eventually, both pains will go away. But what actually is pain? How do you sense it? What makes it go away? In this article, we'll examine the neurobiology of pain, the various types of pain and how pain can be treated or managed.
Pain is the most common reason that people seek medical attention. But pain is actually hard to define because it's a subjective sensation. The International Association for the Study of Pain defines it as an "unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage" [source: International Association for the Study of Pain].
Advertisement
Obviously, this definition is pretty vague. One physician even remarked that pain is whatever the patient says it is. So let's just say that pain is a warning sensation to your brain that some type of stimulus is causing or may cause damage, and you should probably do something about it.
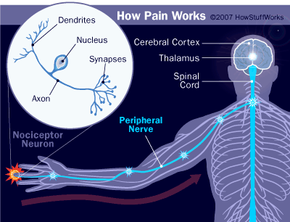
Pain perception, or nociception (from the Latin word for "hurt"), is the process by which a painful stimulus is relayed from the site of stimulation to the central nervous system. There are several steps in the nociception process:
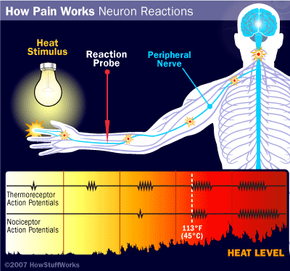
- Contact with stimulus -- Stimuli can be mechanical (pressure, punctures and cuts) or chemical (burns).
- Reception -- A nerve ending senses the stimulus.
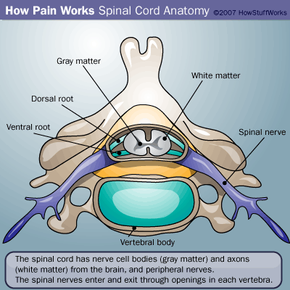
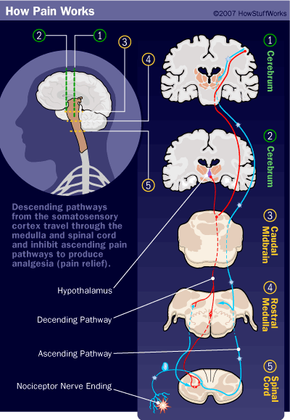
- Transmission -- A nerve sends the signal to the central nervous system. The relay of information usually involves several neurons within the central nervous system.
- Pain center reception -- The brain receives the information for further processing and action.
Nociception uses different neural pathways than normal perception (like light touch, pressure and temperature). With nonpainful stimulation, the first group of neurons to fire are normal somatic receptors. When something causes pain, nociceptors go into action first.
Next, we'll look at your body's nociception pathways.